by Dr A. Mesut Erzurumluoğlu | Principal Bioinformatician at Bicycle Therapeutics (formerly at Boehringer Ingelheim, and Univs. of Cambridge, Leicester & Bristol) – blogging since 2006. All views mine unless stated otherwise
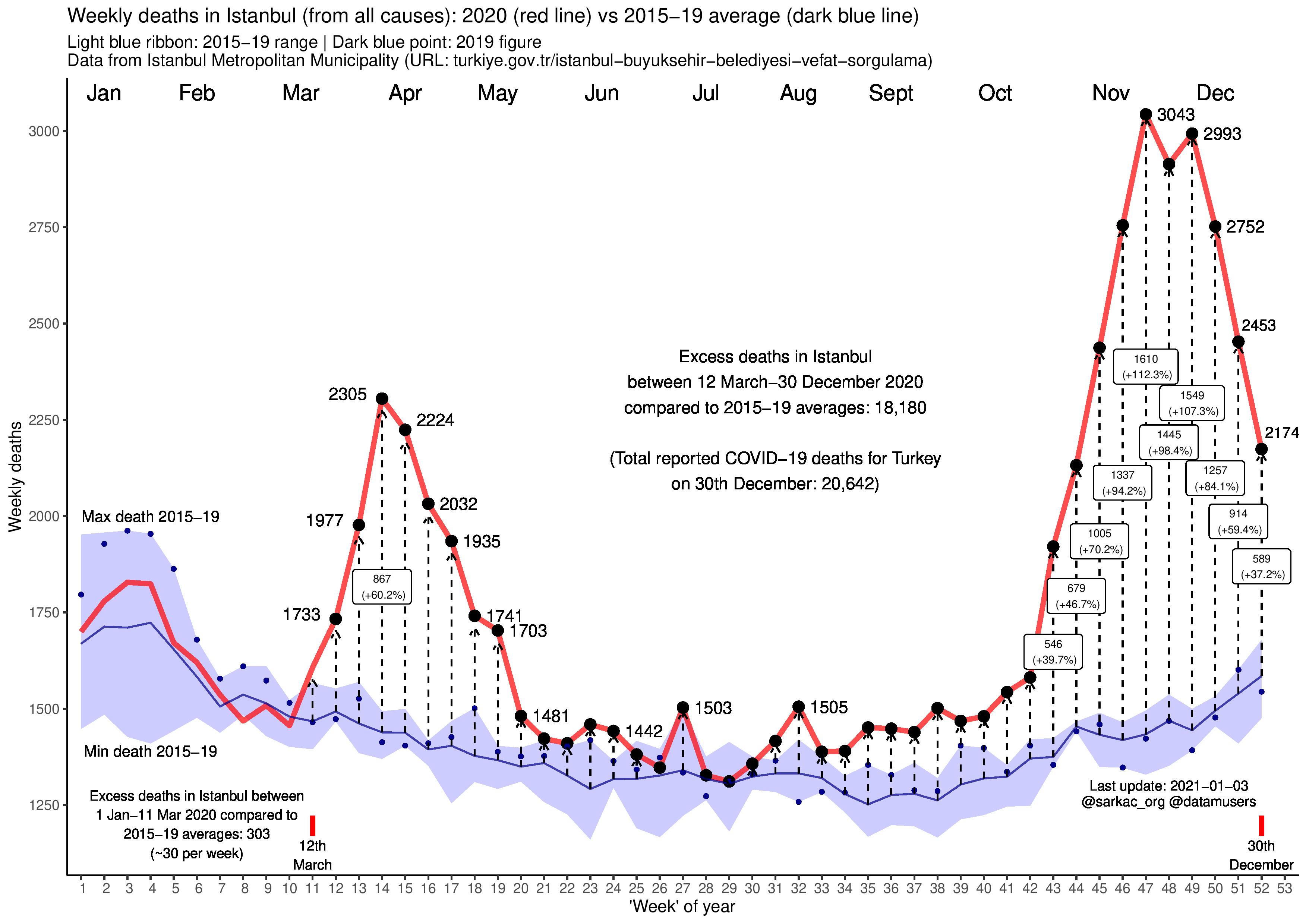
Figure showing excess ‘all-cause’ mortality in Istanbul (Turkey-wide data currently not available) in 2020 compared to 2015-19 averages – up to and including 30th December. We see a sharp increase in the number of excess deaths from week 11 onwards (i.e. 12th March onwards) – the week when the SARS-CoV-2 outbreak seems to have really took off in Istanbul. Reported number of total COVID-19 deaths on 30th December for Turkey was 20,642 (Reported number of total COVID-19 deaths on 25th October for Istanbul was 3,253 – last update; source: Ministry of Health/Sağlık Bakanlığı). But between 12th March and 30th December, we estimate excess deaths in Istanbul alone to be ~18,180 (NB: excess deaths were ~30 per week between 1st January and 12th March). Our estimate most likely points to either/both (i) an underestimation of deaths directly caused by COVID-19 and/or (ii) excessive deaths indirectly related to the current COVID-19 epidemic in Turkey. Both reasons deserve an extensive investigation by the media. Important notes: This figure will be updated and shared on my Twitter feed every few weeks until the end of 2020 (the commentary below – posted 25th May 2020 – will not be updated). The current (red line) plot finishes on the 52nd ‘week’ (i.e. 7-day interval) of 2020 which corresponds to 30th December, but the figures were updated on the 3rd January 2021 because the data provided by Istanbul Metropolitan Municipality is being updated retrospectively – which stabilises after ~7 days. Further details on Istanbul’s death figures can be found here (Mayor of Istanbul’s statement and additional analysis carried out by Financial Times’ analysts) – including details about the initial confusion on whether these figures are ‘burials in Istanbul’ or ‘all deaths in Istanbul’. Plot wholly generated using the ggplot2 library in R.
Prominent newspapers in Turkey (e.g. Cumhuriyet, BirGün, duvaR, T24 – with >1M followers)have picked up on our analysis (incl. commentaries such as: Sınırlı veri, sınırsız pandemi)
Commentary/discussion (25/05/2020)
Excess ‘all-cause mortality’ (that is, deaths from all causes – not just COVID-19) is probably the most informative statistic when comparing countries as there is no standard in reporting COVID-19 deaths between countries (e.g. differential PCR-based testing accuracy, cause of death coded differently e.g. dying with vs due to COVID-19). Premature deaths are also the ultimate outcome to prevent* and easy to measure – making it less likely to be affected by measurement error. Excess all-cause mortality comparisons have their own caveats when comparing all the countries in the world as many countries aren’t transparent even in this regard (e.g. isolated and/or autocratic countries). However, we can still access reliable data from plenty of developed and developing countries – including cities with relatively autonomous local governments (e.g. Istanbul) in countries known to have ‘transparency’ issues.
All-cause mortality statistics can be very useful for acountry/government to analyse how good it is tackling the multi-factorial challenges posed by the epidemic. As is shown in the above figure, analysing excess all-cause mortality will point us to deaths directly and indirectly related to the SARS-CoV-2 epidemic in Turkey. The indirect reasons include (not exhaustive): (i) people being scared to go to hospitals when they should have (and therefore died and not tested), and (ii) when they do, they may not have received the treatment they otherwise would have got due to insufficient number of beds, doctors/nurses.
I really like this figure by the Office of National Statistics (ONS; United Kingdom) as it can be very informative in preventing further unnecessary deaths. An analysis like this can point us to the indirect causes of excess deaths due to the epidemic. For example, there seems to be more people dying of Dementia/Alzheimer disease in England in April 2020 compared to the previous years, thus the causes of this spike should be further looked into (e.g. is it misdiagnosis or due to insufficient treatment?). There also seems to be less dying because of ischaemic heart disease, which probably means some of those who would have died in 2020 because of heart disease died due to COVID-19 – which makes sense as most who have died from COVID-19 were >65 aged men. Turkey (and all countries) should also make this data available. Image source: ons.gov.uk
We should note that (i) 2020’s Istanbul is a relatively less lively city than 2015-19’s Istanbul (e.g. less traffic on the roads and people on the streets) as there have been varying lockdown measures in the last couple of months, and (ii) we do not have access to Turkey-wide data to estimate what the total excess death figure in Turkey is. In our analysis we calculate excess deaths in Istanbul by comparing 2020’s results with 2015-10 averages. So, it is possible that the excess deaths are even higher in Istanbul (and most metropolitan cities around the world). This is something the Turkish government needs to be transparent and open to suggestions/improvement about. They clearly need help but only transparency can ensure that there is minimal unnecessary deaths.
The reasons behind excess deaths and whether the government could have done something about them should also be factored into whether a government is successful or not as very high excess all-cause mortality figures will show that they have tried to tackle this multidimensional problem using narrow-minded approaches. Especially the media need to ask the right questions (e.g. why is Turkey-wide data not available? what are the causes of these excess deaths? what is being done about them? who are advising the Turkish government?).
Aside from current excess deaths, long-term strategies should also be carefully taken – as although current excess deaths maybe low now for some countries (possibly including Turkey – we don’t know for sure), it may end up being as bad as other ‘poorly’ performing countries come the end of 2020 (with the additional ‘double whammy’ of destroying the economy of the country due to stricter lockdown measures). I therefore do not share the view of many academics who are repeatedly calling some countries ‘very successful’ as I think it’s too early to call any country ‘successful’ now. For me, there can only be ‘unsuccessful’ countries at the moment (e.g. Brazil seems to be a clear example of this – unless there are huge changes in policy by the government).
Finally, I value this exercise as I don’t think the media in Turkey is doing a good job of looking into what is causing these additional deaths. I will stop contributing to these analyses once I feel this issue is being properly looked in to by the government and the media**.
I am open to suggestions and criticism regarding these analyses. I am also happy – with appropriate attribution – for anyone to use the figure or the contents of this blog post (including direct Turkish translations).
Thanks for reading!
The official Covid-19 death toll worldwide is above 440,000
But in 27 countries alone, the BBC found at least 130,000 more excess deaths during the pandemic that were not directly attributed to coronavirus
— A. Mesut Erzurumluoğlu (@mesuturkiye) May 25, 2020
Footnotes:
*If I was to provide an extreme example just to prove the point, imagine if whole of the UK was infected (e.g. due there were no lockdowns imposed or the lockdowns didn’t work at all, no education of the public regarding the spread) but there was no deaths from COVID-19 in the country because of world-class treatment provided to all those who were hospitalised, then we could safely say that the UK government/country was very successful. And vice-versa, if the total number of cases was only 100,000 in the whole country but all 100,000 died, then we could easily say – although the lockdowns etc. have worked – that government/country did a terrible job of handling the epidemic.
**There is criticism from some of my Turkish followers on why I’m not doing a similar analysis for the UK (my country of residence). However, similar – and better – analyses have been/are being carried out by scientists and the media professionals for the UK. Needless to say, the media, academia/intelligentsia and civil society in the UK is (i) more inquisitive, and (ii) have considerably more ‘know-how’ than their Turkish counterparts.
PS: Turkish version of the figure will appear on Sarkaç’s Twitter page (@sarkac_org) and blog every week – without the above commentary, as this is solely mine and does not necessarily reflect the views of Sarkaç.
PPS: I’m very concerned about a lack of preparation for an impending (large) earthquake in/near Istanbul. Combining this with more people being at home due to the epidemic, I fear the worst. The government and media must get on this matter as soon as possible.
This is a post inspired by a question I saw online: Which single public health intervention would be most effective in the UK?
I would like to share my own views on the question although don’t expect anything comprehensive as I don’t have much experience about how an idea can be taken further to impact policy and public health practice.
Legend has it that a great chess player travelled to Manhattan to take part in a World Chess tournament. Looking around Central Park, he saw that a crowd had gathered around a street chess player who was offering money to those who could beat him. He decided to give it a go – and after a gruelling match, they shaked hands on a draw. This dented his confidence and ultimately caused him to return to his homeland without taking part in the tournament.
Little did he know that the street chess player was a grand master who wanted to pass time before taking part in the same the tournament.
What has this got to do with a public health intervention? I will come back to it…
From my observations over the last 7-8 years as a scientist studying different common diseases such as diabetes – to which £1 of every £10 of the NHS’s budget is spent on, obesity – which is the major risk factor for heart attacks, and chronic obstructive pulmonary disease (COPD) – currently the third leading killer in the world, it is clear that cheap and effective treatments for these diseases are a long way away. This is not to say that there is no progress as there is tremendous research being carried out on (i) understanding the molecular causes of (e.g. genes, proteins that cause) these diseases and (ii) developing new therapies. The continuous economical costs of treating patients with current state-of-the-art therapies is reaching infeasible levels with a significant proportion being wasted on patients who do not adhere to their prescriptions properly1 and ‘top selling’ drugs being so inefficient that up to 25 patients need to be treated in order to prevent one adverse event such as a heart attack2. These diseases drain the NHS’s budget, cost the lives and healthy years of hundreds of thousands of people and causes emotional distress to the patients and their loved ones. If something is not done now – and quick – latter generations may not have an NHS that is ‘free and accessible to all’ to rely on as the system is already showing signs of failure in many parts of the country3,4 – although costing around 1 in 5 of the government’s annual budget.
Parents need help!
What is also striking about these diseases is that up to 9 in 10 cases are thought to be preventable. Thus, concentrating on prevention rather than ‘cure’ makes most sense as the only economically feasible solution lies here. No single public health intervention is going to solve all the problems that the UK health system faces currently but one thing that has always stared me in the face was how clueless and/or irresponsible most parents are, regardless of which socio-economic stratum they belong to – writing this sentence as I read an article on a teenager who died from obesity after his mother continually brought takeaway to his hospital bed5. The consequence is children living through many traumatic experiences, picking up bad habits and developing health problems due to a combination of ignorance, lack of guidance and toxic environments.
A wise man was once asked: “How do we educate our children?” and he is said to have replied “Educate yourself as they will imitate you”. As a new father, I got to observe first-hand that my child is virtually learning everything in life from myself and my wife. Thinking back, my parents never smoked, did not allow any visitors to smoke in the house, and kept me away from friends who smoked. Their actions were the main factor for myself and my three siblings to never start smoking – although there was pressure from my school friends. Research suggests that this is true across the general population, that is, if parents do not smoke, their children are more likely to become adults who will not either6; if parents prepare healthy food, their children will do too; if parents do not drink or drink moderately, the children will do too; if parents are educated, their children will be too7; and the list goes on… As the only economically feasible hope seems to be prevention, there is no better place to start than educating parents.
Since starting as a researcher at my current institute, I have been to a dozen or so ‘induction courses’, taking lessons on a variety of subjects from ‘equality and diversity’ to ‘fire safety’ to ’unconscious biases’. Although most seemed a bit of a time waster at first, after enrolling to them, I soon accepted that these were important as I did not know how crucial they were in certain situations – situations that are more common than one would think. I would not have attended them if they were not mandatory.
However, arguably, none of these skills that I picked up in these induction courses are as important as being a good parent and helping my children achieve their potential physically, intellectually, psychologically, emotionally and socially. I think it is irresponsible that there exists no mandatory training before people become parents. We as parents are expected to be not just people who keep our children alive by providing for them, but we are also expected to be good dieticians, sleep coaches, pedagogues, psychiatrists, life coaches, friends… Unsurprisingly, many parents are failing horribly as we are not equipped with a solid foundation to guide them properly. The result is: one-third of the population is obese, one-fourth drink above advised thresholds, one-fourth of students report to have taken drugs, one-fifth smoke (noting that vaping is not included in this figure), one-fifth show symptoms of anxiety or depression and up to one-tenth may be game addicts.
To help parents in this long and extremely difficult journey of parenthood, I propose mandatory courses tailored for first-time parents – with exemptions & alternatives available. The specific syllabus and the length of the course should be shaped by pedagogy, public health, psychology, sociology, and epidemiology experts but also by the parents themselves.
In this course parents can:
Be persuaded about the importance of such a course – just as I learned that spending time learning about fire safety was not a bad idea
Be provided with links on where to easily find reliable information (e.g. NHS website)
Learn about the mental and physical health aspects of smoking, drinking alcohol, exercising, eating high sugar content food, pollution, watching TV, reading books, cooking healthy food, mould, asthma triggers, excessive use of social media etc.
Feedback any problems they have to a central panel and make suggestions as to how the course could be improved
Hear about local activities (e.g. ‘Stop smoking’ events, English courses, even events such as Yoga classes)
Receive information about who they can contact if they themselves have addiction problems (e.g. smoking, alcohol, drugs, gambling)
Learn about what to look out for in their children (e.g. any obvious signs of physical and mental diseases, bullying)
Be encouraged to support their children achieve their potential – no matter what background they come from
Be encouraged to offer help in local as well as national problems such as the organ donor shortage, climate change (recycling, carbon emissions), air pollution etc.
Be reminded of the responsibility to provide future generations a sustainable world
Be taught about the relevant laws (e.g. child seat, domestic abuse, cannot leave at home on their own).
I believe if the course is designed with the help of experts but also by parents, the course can be engaging and lead to more knowledgeable parents. This is turn will lead to positive changes in behaviour and a significant drop in the incidence of unhealthy diets/lifestyles, (at least heavy) smoking, substance use and binge drinking – major causes of the abovementioned common diseases. I think to ensure that parents engage and take part in the process, an exam should be administered where individuals who fail should re-take the exam. Parents who contribute to the process with feedback and suggestions can be rewarded with minor presents or a simple ‘thank you’ card from the government itself – a gesture that is bound to make parents feel part of a bigger process. Parents who are engaged in this process will also be encouraged to engage with their children’s education and help their teachers when they start going to school. Parental participation in turn, will positively affect academic achievement and the healthy development of children – a phenomenon shown by many studies8,9. Incentives such as additional child tax credit/benefit and/or paid parental leave for both parents should be considered to increase true participation rates.
These courses can then be accompanied by a number of optional courses where NGOs and volunteers from the local community can offer advice on matters such as ‘how to quit smoking?’, ‘how to find jobs?’, online parenting, English language courses (for non-speakers), and engaging children with local sports teams. I would certainly volunteer to give a session on the genetic causes of diabetes and obesity – and I know there are plenty of academics and professionals (e.g. experienced teachers, solicitors) out there whom would happily offer free advice to those who are interested. There are NGOs providing information on almost all diseases and health-related skills (e.g. CPR, first-aid) and this course would offer a more targeted and cost-efficient platform for them to disseminate their brochures and information on their upcoming events.
Many upper-middle to upper class parents regularly attend similar courses and events – and making this available to every parent would represent another way to close ‘the gap’10. Old problems persist but new ones are added on top such as online gaming, e-cigarettes, FOMO and betting addiction – and the courses can evolve with the times. A government which successfully implements such a course can leave a great legacy as social interventions have long lasting impact and even affect other countries.
One could argue that a course like this should be offered to every citizen at few key stages in their lives (e.g. first parenthood, before first child reaches puberty) – and that would be the ultimate aim. But as this option may initially be very costly and hard to organise and focusing on parents ensures that not only the parents are educated but consequently the children are too – making the process more cost efficient. The first courses could be trialled in certain regions of the country before going nation-wide.
We are all in the same boat – whether we realise or not
I would like to diverge a little to mention the potential sociological benefits of the proposed course: Tolstoy, in Anna Karenina wrote “Happy families are all alike; every unhappy family is unhappy in their own way” – also an increasingly used aphorism in public health circles. However, I observe and believe that many of us are unhappy due to similar reasons: we all want to be listened to, understood and feel like we are being cared about. I believe the proposed course accompanied with an honest feedback system would be a great start in getting the ‘neglected masses’ involved in national issues.
I would like to finish by returning to the little story at the start. I believe that many parents, especially those from poorer backgrounds, give up trying for their children early on as they do not think that they or their children can compete against other ‘well-off’ individuals and therefore see no future for themselves. Their children and grandchildren also end up in this vicious cycle. But if they get to see first-hand in the proposed course that we all – rich and poor – start from not too dissimilar levels as parents and have the same anxieties about our children can also motivate us all to push a little bit extra and hopefully close the massive gaps that exist between the different socio-economic strata in the UK11 – and ultimately decrease the prevalence of the diseases that are crippling the NHS.
Further reading
Shork, N. 2015. Personalized medicine: Time for one-person trials. Nature. 520(7549)
Bluett et al., 2015. Impact of inadequate adherence on response to subcutaneously administered anti-tumour necrosis factor drugs: results from the Biologics in Rheumatoid Arthritis Genetics and Genomics Study Syndicate cohort. Rheumatology. 54(3):494-9
Mike Vuolo and Jeremy Staff. 2013. Parent and Child Cigarette Use: A Longitudinal, Multigenerational Study. Pediatrics. 132(3): 568–577
Sutherland et al. 2008. Like Parent, Like Child. Child Food and Beverage Choices During Role Playing. Arch Pediatr Adolesc Med. 162(11): 1063–1069
Sevcan Hakyemez-Paul, Paivi Pihlaja & Heikki Silvennoinen. 2018. Parental involvement in Finnish day care – what do early childhood educators say? European Early Childhood Education Research Journal, 26:2, 258-273
Jennifer Christofferson & Bradford Strand. 2016. Mandatory Parent Education Programs Can Create Positive Youth Sport Experiences. A Journal for Physical and Sport Educators. 29:6, 8-12
Genetik alanının genel olarak alt-dalları. 15-20 yıl önceki “Genetik”le şimdiki genetik çok farklı ve bir sürü alt-dala ayrıldı. Belki de son 10-15 yılda ortaya çıkan Genetik Epidemiyoloji alanında çalışan ve bütün günü bilgisayar başında geçen bir araştırmacı olarak ben de “genetikçi”yim, tüm günü laboratuvarda geçen ve fare genetiği üzerine çalışan bir araştırmacı da. Not: Yazının genetikle ilgili bölümüne geçmek isterseniz direk “Bu girişten sonra asıl meselemiz olan “genetiğin reklamına” dönecek olursak…” diye başlayan kısma geçin.
Türk (ve Britanyalı) bir bilim insanı olarak halkımızın bilimle fazla ilgilenmemesine çok kızıyorum. Hatta akademisyenlerin/araştırmacıların dahi fen bilimleri ve/ya da sosyal bilimlerden çok siyasetle içli-dişli olması beni çıldırtıyor ve ülkem adına ümidimi kaybediyorum. Fakat kendi kendime “bir bilim insanı olarak bunun değişmesi için neler yapıyorum?” diye düşündüğümde haftada bir gün birkaç Türk gence özel fen/matematik/ingilizce dersi vermenin ve sağda-solda gençlere verdiğim konuşmaların dışında fazla birşey aklıma gelmiyor. Bunun üzerine “belki bir-iki kişi okur/çocuklarıyla paylaşır” düşüncesiyle bilimin her türlüsünün, özellikle de genetiğin reklamını yapan bir blog yazısı yazmaya karar verdim. Genel olarak bilim üretmenin önemi üzerine fikirlerimi sunduktan sonra, kendi alanım olan Genetik/Genetik Epidemiyoloji’ye doğru bir geçiş yapacağım. Kendim de nispeten genç ve daha yolun başında olduğum için (yaş 30) sözlerim daha çok lisans öğrencisi ve üniversite-öncesi yaşlardaki arkadaşlara yönelik olacak; hızlıca yazdığımdan daha olgun okurlarım için çiğ bir yazı olarak görünebilir. Ayrıca, istediğimden uzun bir yazı oldu maalesef. Isterseniz sonraki iki paragrafı okumadan direk “Bu girişten sonra asıl meselemiz olan “genetiğin reklamına” dönecek olursak…” diye başlayan kısma geçin.
Belki sıkıcı, yavan ve klişelerle dolu olacak ama önemli gördüğüm bir girişle başlayayım: Tüm gün siyaset, futbol/dizi ve komplo teorileri hakkında konuşan milletlerin, tüm insanlığı geçtim, kendi ülkelerine dahi bir fayda sunmaları imkansız. Bu milletler bir süre ülkenin kendi yeraltı/üstü kaynaklarından faydalanıp, onları tükettikten sonra, her alanda dışa bağımlı olmak zorunda kalırlar. Maalesef, Türkiye de bu konuda epey bir yol kaydetmiş durumda: Teknoloji, tıp ve diğer önemli bilim alanları adına çok birşey üretmediğimizden dolayı, hemen hemen her ilaç, teknoloji ve sistem/bilgiyi dışarıdan ithal ediyoruz. Haliyle belki 5 liraya üretilen elektronik eşya/sistem/ilacı 100 liraya satın alıyoruz. Ayrıca, o kadar para harcamamıza rağmen, “know-how”, yani bir işi düzgün bir şekilde yapabilme ve daha da geliştirebilme özelliğini de kazanamıyoruz. İşler böyle gittiği sürece de ilelebet fahiş fiyatlar ödemek zorunda kalacağız. Devlet insanına ve bilime (research & development) yatırım yapmadığından, ülkenin ekonomik olarak alım gücü zayıfladığı an, büyük krizler kapıdan içeri girecek ve normalden de daha büyük tavizler vermeden, bir sürü maddi-manevi sıkıntı çekilmeden ve on yıllar kaybedilmeden aşılamayacak. Özellikle biriken borçlarla gelecek nesillerin emekleri ve imkanları çalınacak. Bilimin önemine en güzel örnek iki tane dünya savaşı geçirip, ikisinde de düşman tarafından dümdüz edilmiş Almanya’nın nispeten kısa bir sürede kendine gelmesi ve şu anda dunyanın en büyük teknoloji, ilaç ve bilim üreten ülkesi olması – çünkü (dünyanın her yerinden gelmiş) bilim insanlarını baş üstünde tutan bir millet. Tüm dünya ekonomik krizle boğuşsa dahi, kendi başına ayakta kalabilecek belki de tek ülke. Bilim insanlarına atalarının yaptığı hataları analiz ettirdikten sonra, aynı hataları tekrarlamadan yollarına devam etmişler. Hem sosyal olarak, hem de teknolojik olarak gelişmişler. “Bizim atalarımız hata yapmaz” bağnazlığından kurtulup (örnek: Kemalisti de, Islamcısı da, Ulkücüsü de tiksindirici şekilde geri kafalı bu konuda), bu savaşları çıkaran ve ülkeyi her türlü krize sokan nesillere ise lanet okuyorlar. Almanya o günlerde olanlardan dolayı hala bazı ülkelere tazminat ödüyor. Biz de ise başımıza ülke olarak gelen olaylar bilimsel olarak araştırılmadığından tarih hep tekerrür ediyor – hep aynı hatalar, aynı krizler…
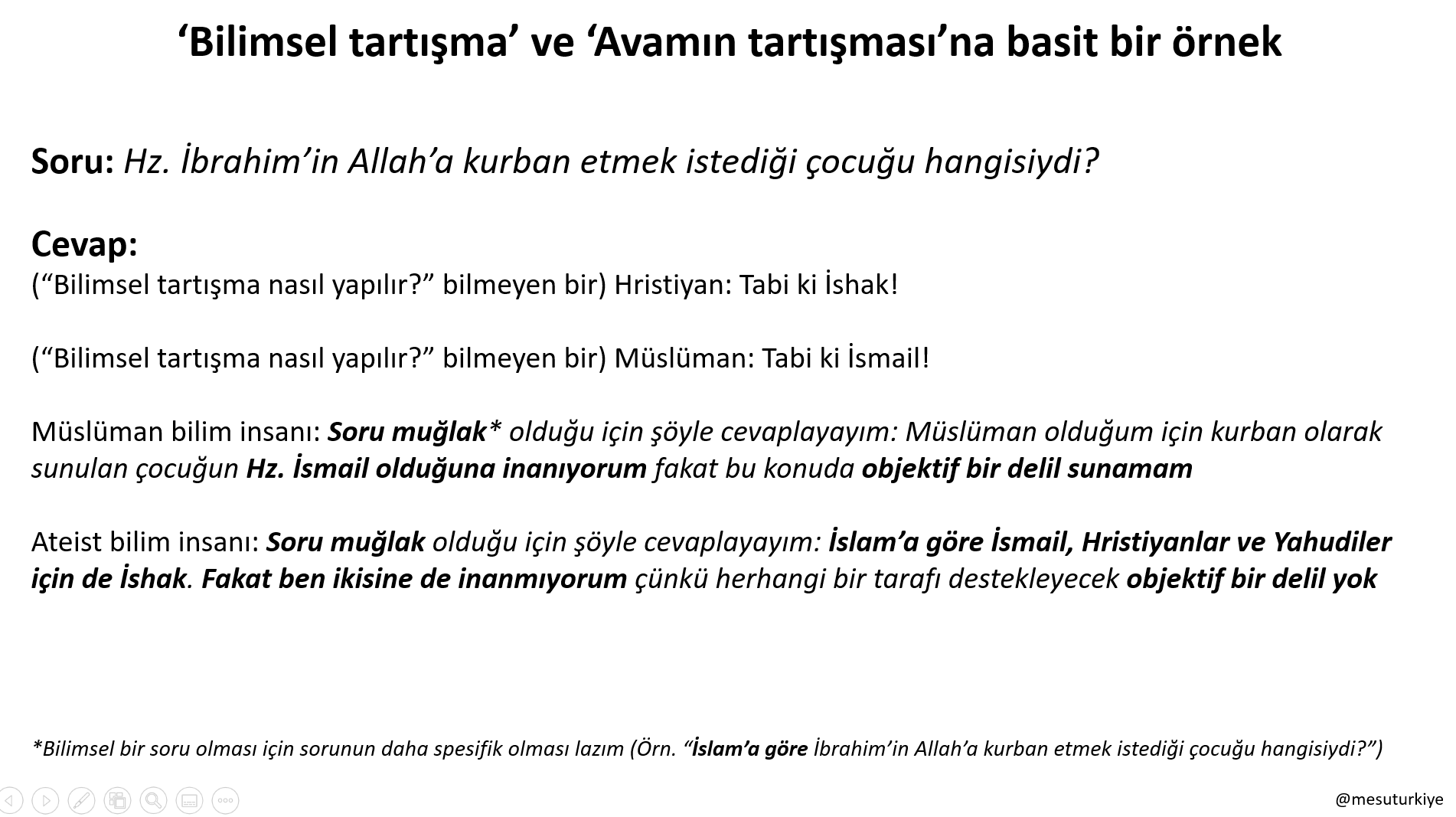
‘Bilimsel tartışma’ ve ‘Avamın tartışması’na basit bir örnek. “Bilimsel tartışma nasıl yapılır?” bilmeyen bir insanın hayata bakışıyla, bilmeyen arasındaki farkı az/çok ortaya koyuyor…
Bunları yazmamın sebebi ise eğer bilim insanı olmanın çok da önemli olmadığını düşünüyorsan, yanıldığını hatırlatmak içindir – her ne kadar da arkadaşlarının hepsi futbolcu olmak istese ya da etrafındaki insanlar tüm gün futbol/dizi hakkında konuşsa da… Bana göre bilim insanları dünyanın en çok ihtiyacı olduğu grup. Büyüdüğünde bakarsın: değerin Türkiye’de anlaşılmazsa, Amerika, Almanya, Ingiltere gibi dünyanın en gelişmiş ülkelerindeki gruplar değerini bilecektir. Gelişmiş dünyada her zaman iş bulabilecek bir insan olacaksın. Hele bir de her akademik grubun ihtiyacı olan bir yeteneğe sahipsen (fen bilimleri için genel bir örnek: ‘big data’ analiz/data science, sağlam istatistik bilgisi). Bu fırsatı başka hiçbir iş alanında kolay kolay bulamazsın. Ayrıca dünyaya ve hayata karşı bakışın ise çoğu insandan daha farklı ve kapsamlı olacak. Bu ise bana göre bir insanda paha biçilmez bir özellik. Hayatta sadece bilim insanlarının gördügü düzen ve desenler var ve bunların en azından bir kısmını görmeden ömür tüketmek çok büyük bir kayıp. Bu konuyu önceden paylaştığım Entelektüeller neden sevilmezler?, Din, bilim ve bilim adamları ve Duya duya gına geldi arkadaş gibi yazılarıma havale ediyorum. Özetle, ileride bir “bilim insanı” olmanızı tavsiye ediyorum.
Bir insanda 50-100 trilyon (100,000,000,000,000) hücre var (bunların %90’ı bakteri) ve inanılmaz bir şekilde, bir ignenin ucundan bile onlarca kat küçük olan (insan) hücrelerinin her birinin içinde yaklaşık 2 metre uzunluğunda DNA bulunuyor. Image source: fenogretmeni.net
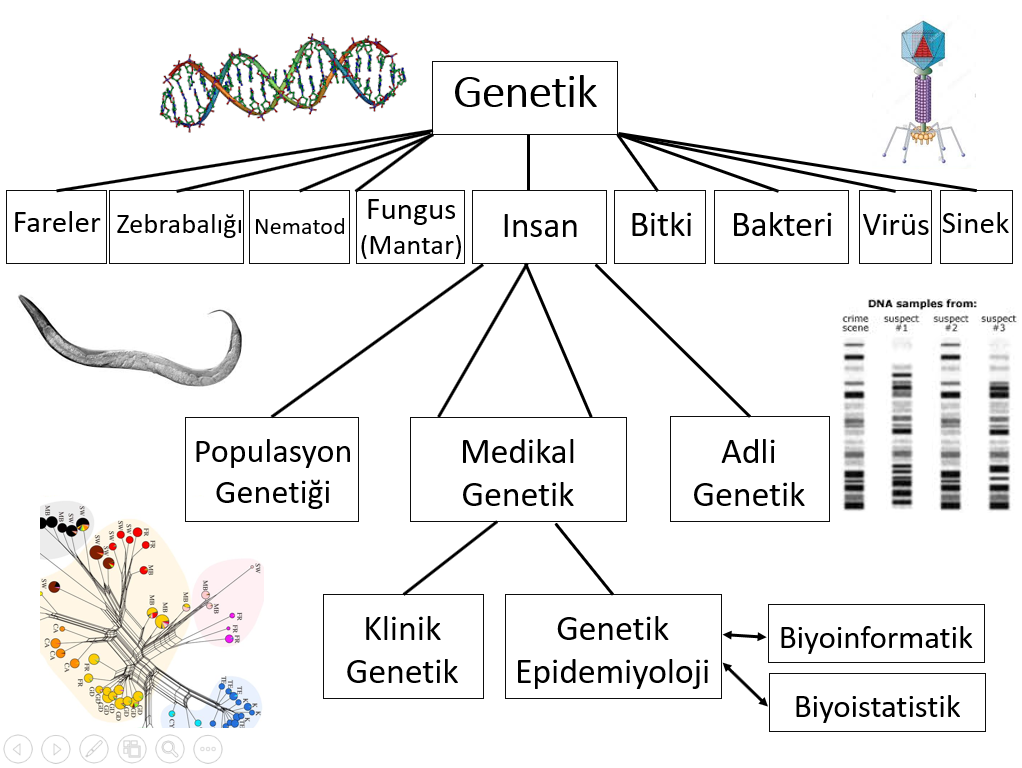
Bu girişten sonra asıl meselemiz olan “genetiğin reklamına” dönecek olursak: ben çocukken genetik “geleceğin mesleği”ydi. İşin garibi şu anda da geleceğin meslekleri arasında yer alıyor. Fakat ufak bir farkla: ben çocukken, “çocukken” dediğim de daha 15 sene öncesi, genetik alanı çok genel olarak “insan genetiği/klinik genetik”, “model organizma ve hayvan/bitki genetiği” ve “adli genetik” olarak üçe ayrılıyordu ve çoğunlukla genetik denince akla beyaz önlüklü, laboratuvarda çalışan ve ufak tüplerde bazı sıvılar karıştırıp bunları değişik jellere yerleştiren insanlar akla geliyordu. Şimdi ise laboratuvarda çalışan insanlar hala olsa da, artık genel olarak laboratuvardaki işler kolaylaştığından, beyinden daha çok el mahareti önemli hale geldi ve tabir-i caizse, bu tarz “ayak işlerini” çoğunlukla akademisyen/araştırmacı olmayan “teknisyen”ler yapıyor. Akademisyenler/araştırmacılar ise asıl beyin gerektiren işlerle uğraşıyorlar ve her işlerini artık bilgisayarda hallediyorlar. Örneğin ben DNA fingerprinting’in (DNA parmak izinin) bulunduğu Leicester Üniversitesi’nde Kronik Obstrüktif Akciğer Hastalığı (KOAH) üzerine çalışan bir Genetik Epidemiyologum ve kariyerim boyunca, doktora projemin ufak bir bölümü dışında hiç laboratuvarda çalışmadım – laboratuvarda çalışmayı da hiç sevmedim. Şu anda bir araştırma görevlisi (Postdoctoral Research Associate) olarak günlük işim yüzbinlerce insanın genetik (kişi başı milyonlarca mutasyona/genetik varyanta tekabül ediyor) ve (kişinin yaş, cinsiyet, sigara içip-içmediği gibi) fenotipik datasını “süper bilgisayar”ları kullanarak istatistiki olarak analiz etmek. Bu sayede insanları KOAH’a meyilli hale getiren genleri ve varyantları tespit etmeye ve bulduğumuz genlerin arasından biri “bir KOAH ilacına netice verir mi?” diye araştırmaya çalışıyoruz. Ayrıca yaptığımız analizlerden ne çıkacağı belli olmadığı için her sabah işe kalktığımda “ya Hu yine mi iş?” diye iç geçirmiyorum. Bir buluş yaptığımız zaman ileride insanlara bir ilaç olarak dönebileceğini düşünmek ise insanı manevi olarak mutlu ediyor. Genetik Epidemiyoloji alanı, diger alanlar gibi, çok hızlı ilerlediğinden belki her hafta ses getiren bir makale çıkıyor ve onları okuyunca insanın içi açılıyor ve geleceğe dair bazı hastalıkların tamamen tedavi edilebilmesi adına umudu artıyor.
Bir ‘Circos’ çizimi (Circos plot). Teknik detaylara fazla girmeden, bu çizimde genomumuzda hangi bölgelerin KOAH tanısı için kullanılan FEV1, FVC ve FEV1/FVC’yle istatistiki olarak korelasyon gösterdigini görebiliyoruz. Çizimde bulunan her nokta – milyonlarca var – DNA’mızda bir varyanta tekabül ediyor ve noktalar yüksekse, orada bulunan genlere (isimleri dış dairede) sonraki araştırmalarımızda öncelik veriyoruz.
Bunları anlatmamın sebebi ise, diyelimki, lisede notların iyi ve üniversitede genetiği kazanma hakkı kazandın ama “kariyer olarak genetiği sevecek misin?” tam bilmiyorsun. Şimdiden sana seveceğini söyleyebilirim. Çünkü ilk figürde de göreceğin gibi genetik o kadar büyük bir alana dönüştüki Avrupa ve Amerika’da artık birçok üniversitenin Genetik departmanı Biyoloji departmanından ayrı. “Saf genetik” diye bir alan artık yok denebilir – çünkü genetiğin bir sürü birbirinden çok uzak alt-dalı (sub-field) oluştu. Bu yüzden ben de “genetikçiyim” dediğimde aslında işin kolayına kaçıyorum demektir. Genetik alanını bilen birisi bana “tamam da; genetikte hangi alandasın?” diye sorar çünkü başka bir “genetikçi”yle çok farklı konuları çalışıyor, çok farklı teknikler kullanıyor olabiliriz. Bu yüzden genetiği seçtikten sonra kendi kendine düşünmeli ve şimdi sıralayacağım alt-dallardan birine doğru ilerlemelisin:
Eğer, daha çok çocuk yaştayken ortaya çıkan, Kistik fibroz (Cystic fibrosis) ve Akdeniz atesi (Mediterranean fever) gibi 100% genetik hastalıklar üzerine çalışmalar yürütmek istersen Klinik Genetik* (Clinical Genetics) alanını düşünebilirsin;
Benim şimdi yaptığım gibi kanser, diyabet, obezite, KOAH gibi daha kompleks (hem genetik, hem sigara/alkol/hava kirliliği gibi çevresel etkenlerin önemli olduğu) hastalıkları çalışmak ve potansiyel olarak milyonlarca insanın hayatına katkı sağlama fikri hoşuna gidiyorsa Genetik Epidemiyoloji;
CSI (Crime Scene Investigation) dizisindeki gibi cinayetlerin çözümünde yer almak istiyorsan Adli genetik (Forensic genetics);
İnsanlık tarihini etkileyen eski caglardaki büyük savaşlar, göçler gibi olayları genetik ve tarihsel olarak çalışmak istiyorsan Popülasyon genetiği (Population genetics);
İnsanlar üzerinde genetik deneylere izin verilmediği için insanlardaki bazı gen/protein/biological pathway’lerin üzerine çalışmak adına (insana genetik olarak en cok benzeyen hayvanlar olan) maymun, (fizyolojik olarak insanlara çok benzedikleri ve maymunlar üzerinde calışmaya nazaran daha ucuz ve etiksel oldukları için) fare/sıçan (murine), yuvarlak kurt (nematode), sirkesineği (Drosophila melanogaster) ya da zebrabalığı (developmental biology/gelişim biyolojisi) genetiği;
Bakteriler ve menenjit gibi bakteriyel enfeksiyonları çalışma adına Bakteri genetiği (Bacterial genetics);
Virüsler ve grip virüsü gibi virüslerle ilgili enfeksiyonlarını çalışma adına Virüs genetiği (Viral genetics);
Mantarlar ve kandidiaz gibi enfeksiyonları çalışma adına Mantar genetiği (Fungal genetics);
Bitkiler üzerine çalışmak ve/ya da insan nüfusu arttığı için ileride yemek bulmanın problem olmaması adına bitkilerin verimliliğini arttırmak istiyorsan Bitki genetiği (Plant genetics);
Eski canlılar üzerine çalışmalar yürütmek istersen Paleogenetik (Palaeogenomics);
Canlıların evrimi üzerine çalışmak istersen (ilk figürde olmayan) Evrimsel genetik (Evolutionary genetics)
Çok büyük genetik dataların en iyi şekilde analiz edilmesini ve anlaşılmasını kolaylaştırmak istersen Biyoistatistik (Biostatistics) ya da
Biyoenformatik (Bioinformatics)
alanlarında çalışabilirsin. Ayrıca, yeni dönemde (büyük ihtimalle bu sistemi bulanlara Nobel kazandıracak) CRISPR-Cas9 tekniğiyle insan genlerini dahi editlemeye/düzenlemeye başlayacaklar ve bir sürü hastalığı meydana getiren mutasyonları insanların genomlarından silecekler. Klonlamadan, kök hücre teknolojilerinden, gen terapilerinden, epigenetikten vs. hiç bahsetmedim bile. Yukarıda bahsettiğim her alt-dalda inanılmaz gelişmeler oluyor ve bu yüzden bana göre genetik alanı içinde her tür insanın beğeneceği bir alt-alan bulunabilir. Bulamıyorsan, iyi araştırmıyorsun demektir.
Bu yazımda “genetikçi” (aslında genetik epidemiyolog) olduğum için genetiğin alt-dalları üzerine detaylar verdim ve reklamını yaptım ama yukarıda söylediklerim artık birçok sosyal bilim ve fen bilimi için de geçerli**. Fakat büyük devletler genetik ve biyokimya alanına çok büyük paralar akıttığı için iş ve çalışacak proje bulma sıkıntısı çekmeyeceksiniz.
Umarım biraz fedakarlık yapıp, bilim insanı olmaya karar verirsiniz; çünkü halkımızın siyasetin kısır döngüsünden kurtulmasını bana göre ancak bilim insanları ve entelektüeller sağlayabilir. Ama binde birlerden yüzde birlere çıkması ve onlara karşı bakış açısının değişmesi ve önemlerinin artması lazım. Tabi genetik alanına girmeye karar verirseniz ekstradan mutlu olurum. Umuyorumki fikir dünyanızın gelişmesiyle doğrudan etrafınızdaki insanlara ve öğrencilerinize; yazdığınız kaliteli makalelerle ise tüm insanlığa faydanız dokunacak.
Gelecek sorulara vs. göre bu tarz yazıları yazmaya devam etmek istiyorum. Okuduğunuz için teşekkür ederim.
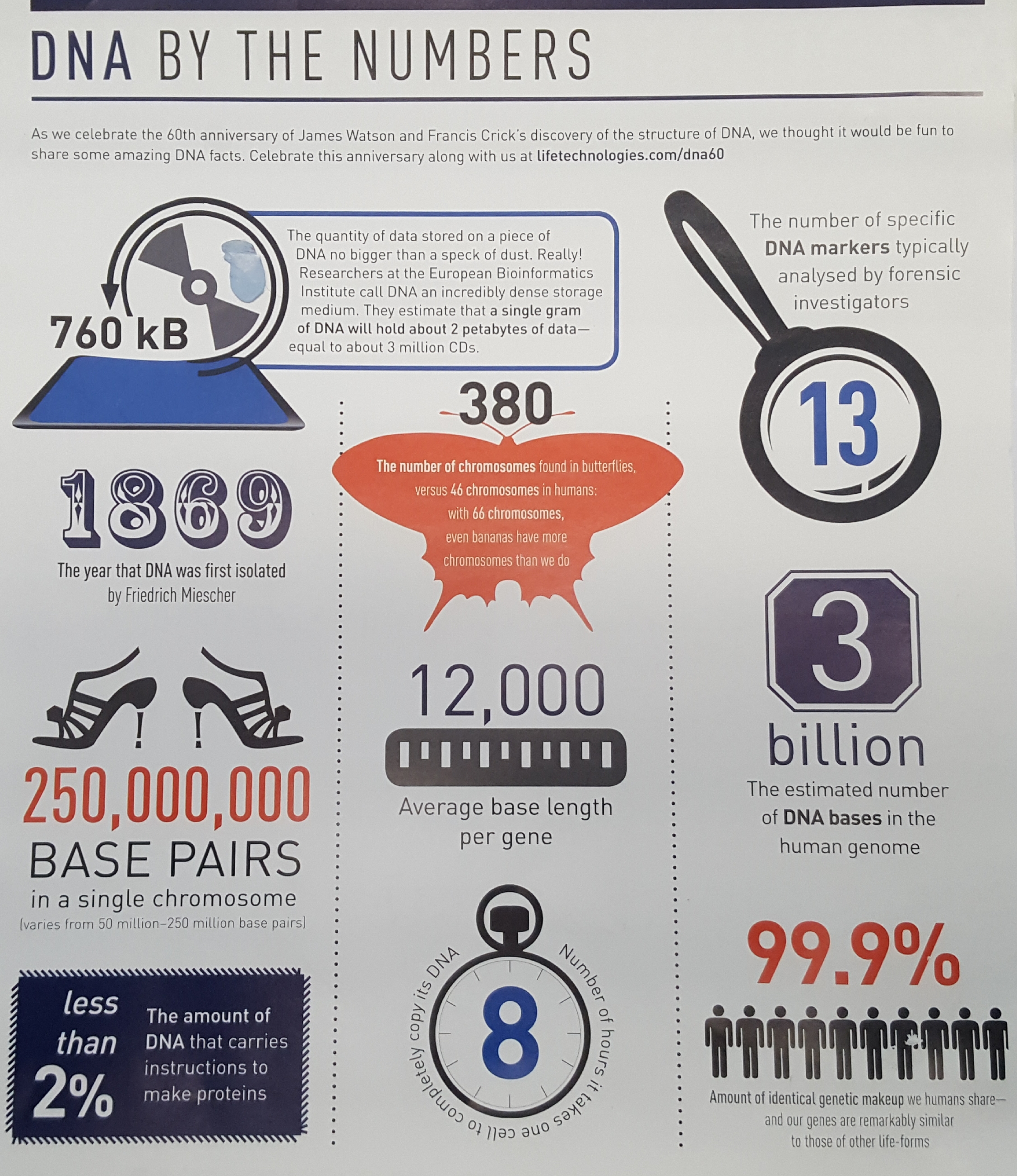
DNA’yla ilgili ilginç anektodlar (‘DNA by the numbers’ by Life Technologies)
*Doktoramda Suudi Arabistan’daki akraba evlilikleri üzerine çalışmıştım ve yaptığım çalışmalar daha çok Klinik genetik alanına katkı sağlamıştı. Şimdi ise Genetik Epidemiyoji alanındayım. Makalelerime Google Scholar hesabımdan bakabilirsiniz.
Epidemik haline gelebilecek hastalıklar. Bunların herhangi birine çare buldugumuz vakit, milyonlarca insanın hayatını kurtarmış olacagız. (‘Emerging Threats’ graphic by Nature. Source URL: http://www.nature.com/news/how-to-beat-the-next-ebola-1.18114)
Breathtaking genes: A ‘Circos’ plot depicting how chronic obstructive pulmonary disease (COPD) has become a global concern – the 3rd biggest killer, defined by poor lung function. Our work shows that many parts of our DNA play a role in our lung health. Peaks in red are newly discovered regions, and the blue ones were previously identified by other groups. Millions of genetic variants from tens of thousands of individuals were analysed in this study. The identified genes will help us understand why some of us have better lung function, and lead to the identification of drug targets of potential relevance to COPD.
A press release was issued by the University of Leicester Press Office on 6 February 2017 about a study that I was also heavily involved in (please click on links below for details):
The study has received a lot of attention from the media, with articles appearing in large media outlets such as BBC News, The Independent and MSN News. If you’re interested in the details, please read the paper published in Nature Genetics.
If interested in reading about the area of Genetic Epidemiology itself, please have a look at my (previously published) blog post about the matter: Searching for “Breath taking” genes. Literally!
Details on Circos plot* (above): FEV1: Forced expiratory lung volume in 1 second; FVC: Forced lung volume capacity; FEV1/FVC: the ratio of the two measurements. Labels in the outer circle show the name of the nearest gene to the newly identified (red) variants. X-axis: Genomic position of variant in genome (chromosome number in the outer circle), Y-axis: Statistical significance of variant in this study (higher the peak the greater the significance).
*The figure is a more artistic version of Figure 1 (Manhattan plot) in the above mentioned academic paper. It did not make it into the final manuscript published in Nature Genetics (6th Feb 2017) as it was found to be “confusing” by one of the reviewers – and the editor agreed. 😦 However, the plot was shortlisted (title: Breathtaking genes) and displayed in the Images of Research exhibition (9th Feb 2017) organised by the University of Leicester. 😉
My role in the Wain et al paper mentioned above: I led the ‘functional follow-up’ of the identified associated variants (e.g. mining eQTL datasets, biological pathway analyses, identify druggable genes, pleiotropy, protein-protein interactions) and appropriately visualise the GWAS results (various Manhattan and Circos plots). I was part of the core bioinformatics team of three in Leicester – alongside Dr. Nick Shrine and Dr. Maria Soler-Artigas.
References:
Wain LV et al., Published online 6th Feb 2017. Genome-wide association analyses for lung function and chronic obstructive pulmonary disease identify new loci and potential druggable targets. Nature Genetics. URL: https://www.nature.com/articles/ng.3787
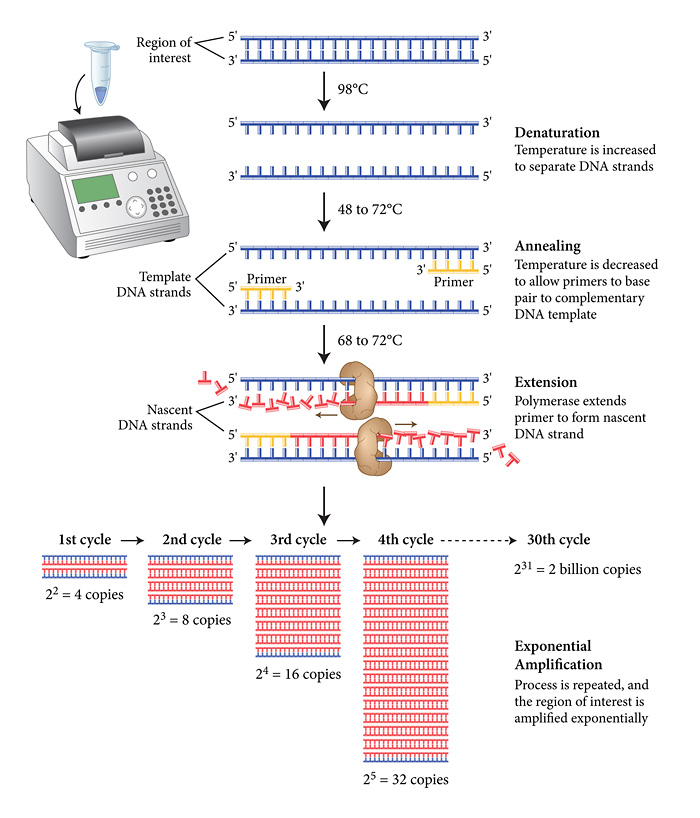
Schematic of the PCR (Polymerase Chain Reaction) process – a technique used to amplify a specific region of DNA. Source URL: http://www.neb.com
This is a very quick guide to designing a primer for PCR (Polymerase Chain Reaction) which will be used to amplify a region of interest. The produced amplicons can then be sent to companies such as GATC-Biotech (located in Germany) to be sequenced. I have seen many blogs with this title but none of them guide you in the way you would expect them to. So I decided to write my own to hopefully make things easier for you:
(i) To design a primer, first click on the link below:
(ii) On the Primer Blast page, you will come across the ‘PCR Template’ box at the top. Enter the ‘Accession ID’ of your transcript of interest from RefSeq if you’re working with mRNA.
If you’re interested in amplifying a genomic region then use Ensembl by (i) searching for your gene of interest on the Ensembl homepage; (ii) then clicking on your gene of interest in the results; (iii) then in the ‘Gene’ view, clicking on the ‘Sequence’ in the ‘Gene-based display’ on the left; and (iv) then by copying the ‘Marked-up sequence’ in FASTA format and pasting it into the ‘PCR Template’ box.
Calculate where your variant of interest is located in the FASTA sequence (Ensembl) or in the transcript (RefSeq mRNA) you pasted and fill in ‘Forward Primer’ and ‘Reverse Primer’ accordingly. I’d advise having a flanking region of ~150bp on both sides of your variant (e.g. if your variant is located at position 500 in your FASTA sequence, then type 350 into ‘From’ in ‘Forward Primer’ and 650 into ‘To’ in ‘Reverse Primer’, leave the other two empty).
(iii) In Primer Parameters:
To get the amplicon sent and sequenced at a company, keep the PCR product size manageable (e.g. 150bp to 300bp).
(iv) If working with human genomic data, change ‘Database’ to ‘Genome (reference assembly from selected organisms)’ and select ‘Homo sapiens’ as ‘Organism’ in ‘Primer Pair Specificity Checking Parameters’.
Click ‘Advanced parameters’.
(v) Change ‘Primer Size’ in ‘Primer Parameters’ to 18 (min), 22 and 25 (max) respectively.
Change ‘Primer GC Content (%)’ to 40.0 and 60.0 respectively.
Change ‘GC Clamp’ to 1.
Change ‘Max Poly-X’ to 3.
Tick the ‘SNP handling’ box (important!).
(vi) Scroll to bottom and click ‘Show results in a new window’ before clicking ‘Get Primers’.
(vii) Wait for results and select a couple* of primer pairs and test them in an in-silico PCR software (e.g. UCSC In-Silico PCR) – designing at least two primer pairs is important; in case one fails, the other one usually works.
(*check that the GC content of the forward and reverse primers are similar to each other for each primer pair.)
Once you’re happy with the amplicons produced in the in-silico PCR program (e.g. your variant** of interest is located towards the centre of the amplicon as desired) then check for hairpin formation (both for forward and reverse primer, separately) using a software such as OligoCalc.
(**if your gene of interest is on the reverse strand, then you would have to use software such as Reverse Complement to change the sequence of your amplicon to its complement so that it matches the Ensembl gene sequence that you’re comparing it against – where you obtained the sequence in FASTA format in step ii).
Once your primer pairs pass all these tests, order them from a company such as Eurofins.
When performing PCR, choosing the annealing temperature may not be straightforward. Although there is a formula for calculating optimum annealing temperature (Ta; see link), (for primers with no unintended targets***) I usually set it 6-7 Celsius below the melting temperature (Tm; you should have received this info from the company that you ordered the primer from) of the primer with lowest Tm. However Ta and MgCl2 gradients/titration may be needed sometimes if PCR doesn’t seem to work for both of the primers you designed earlier.
Sometimes the polymerase used may also need to be changed. So if conventional Taq polymerase doesn’t seem to work (or produces too many unwanted targets), trying a Hot Start activated polymerase (which is way more expensive) could be the answer.
(***if there are other unwanted bands in the gel, try increasing Tm as this will allow the primer to hybridize to the perfectly matching DNA sequence and not to the other unintended regions (which will hopefully be the region you wanted, if you designed the primer well)…
Hope it helps. I’m happy to answer any questions you may have. PCR is a dark art and anything can go wrong! Just need to keep trying 😉
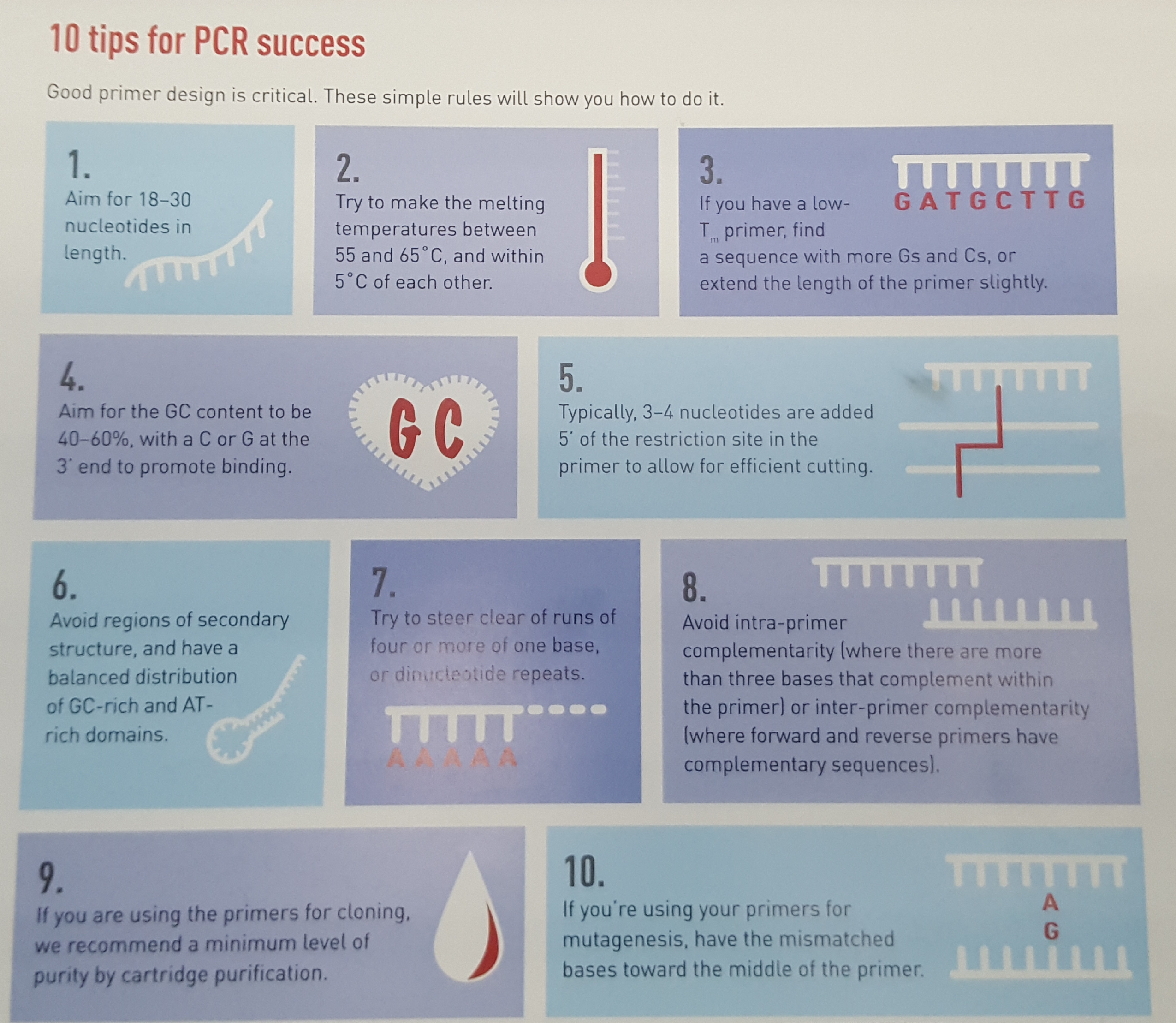
10 Tips for successful PCR primer designing (by Life Technologies)
PS: I have no conflicts of interest and have no connections to either Eurofins or GATC-Biotech
Ben 12 yaşındayken (2000) ailecek İngiltere'ye taşındık ve ingilizcem neredeyse sıfırdı. Bunu duyan (Karen Holman adında) Sınıf Öğretmenim, kendimi evimde hissedeyim diye tüm arkadaşlarıma Türkçe cümleler dağıtmış. Sınıfa girer-girmez arkadaşlarımın hepsi bana "Hoşgeldin" dediler








{kind=link}