by Dr A. Mesut Erzurumluoğlu | Principal Bioinformatician at Bicycle Therapeutics (formerly at Boehringer Ingelheim, and Univs. of Cambridge, Leicester & Bristol) – blogging since 2006. All views mine unless stated otherwise
I worked on rare genetic diseases during my PhD and looked for novel disease causal genes – which I was lucky enough to find1. I also became familiar with the state of rare disease therapeutics: there over 7,000 rare diseases for which only %5 have therapies2. A large majority of rare diseases are neglected by Pharma companies most probably as the market is not as big as it is for common diseases (e.g. obesity, diabetes, COPD). Thus, when I was approached by an old family friend out of the blue and told that his 11 month-old son was a spinal muscular atrophy (SMA) type 1 patient, I straight away thought “the child probably has no hope“.
I did not mention the lack of therapies for rare diseases to my friend and did some research about SMA – a severe neuromuscular disorder where many patients die before the age of two. I was surprised to see that there was an apparently effective ‘cure’: Zolgensma, a gene therapy/drug that Novartis are offering for ~$2.1 million – the world’s most expensive drug at present. Although the drug is FDA and EMA approved, the NHS does not offer the drug at the moment as it has not been reviewed by the NICE committee – which thoroughly reviews all credible drugs and advises the NHS on whether to offer it to UK patients or not.
As we saw that quite a few parents ran successful crowdfunding campaigns and got their children to have the therapy, we decided to do the same (Metehan’s Gofundme page). As the crowdfunding campaign gathered pace, I was sent a tonne of emails – including the academics listed below – asking how Novartis can charge such a price for one drug. While we understand that this is not just a quest for profits and the price reflects R&D and production costs as well as Zolgensma’s position compared to competitors such as Spinraza (Biogen) – offered by the NHS, which is thought to cost around ~£400,000 per patient (real price unknown due to undisclosed agreement3) for just the first year – we believe that Novartis should provide a breakdown of what the profit margin of Zolgensma is per patient.
While we commend Novartis and other companies for investing in rare diseases and can only hope more would follow suit, disclosing profit margins would be most ethical thing to do, which in turn can provide a room for negotiation for patients, and low and middle-income countries (LMIC).
Dr A. Mesut Erzurumluoglu, Research Associate/Genetic Epidemiologist (MRC Epidemiology Unit, University of Cambridge)
Signed by:
Dr Zeynep Hulya Gumus, Assistant Professor of Genetics and Genomic Sciences (Icahn School of Medicine, Dept. of Genetics and Genomics)
Dr Sevinc Ercan, Associate Professor of Biology (New York University, Faculty Director of Diversity, Equity and Inclusion)
Prof. Cem Say, Professor of Computer Science (Bogazici University, Dept. of Computer Science)
Tambuyzer, E. et al. Therapies for rare diseases: therapeutic modalities, progress and challenges ahead. Nature Reviews Drug Discovery19, 93-111 (2020).
This is a post inspired by a question I saw online: Which single public health intervention would be most effective in the UK?
I would like to share my own views on the question although don’t expect anything comprehensive as I don’t have much experience about how an idea can be taken further to impact policy and public health practice.
Legend has it that a great chess player travelled to Manhattan to take part in a World Chess tournament. Looking around Central Park, he saw that a crowd had gathered around a street chess player who was offering money to those who could beat him. He decided to give it a go – and after a gruelling match, they shaked hands on a draw. This dented his confidence and ultimately caused him to return to his homeland without taking part in the tournament.
Little did he know that the street chess player was a grand master who wanted to pass time before taking part in the same the tournament.
What has this got to do with a public health intervention? I will come back to it…
From my observations over the last 7-8 years as a scientist studying different common diseases such as diabetes – to which £1 of every £10 of the NHS’s budget is spent on, obesity – which is the major risk factor for heart attacks, and chronic obstructive pulmonary disease (COPD) – currently the third leading killer in the world, it is clear that cheap and effective treatments for these diseases are a long way away. This is not to say that there is no progress as there is tremendous research being carried out on (i) understanding the molecular causes of (e.g. genes, proteins that cause) these diseases and (ii) developing new therapies. The continuous economical costs of treating patients with current state-of-the-art therapies is reaching infeasible levels with a significant proportion being wasted on patients who do not adhere to their prescriptions properly1 and ‘top selling’ drugs being so inefficient that up to 25 patients need to be treated in order to prevent one adverse event such as a heart attack2. These diseases drain the NHS’s budget, cost the lives and healthy years of hundreds of thousands of people and causes emotional distress to the patients and their loved ones. If something is not done now – and quick – latter generations may not have an NHS that is ‘free and accessible to all’ to rely on as the system is already showing signs of failure in many parts of the country3,4 – although costing around 1 in 5 of the government’s annual budget.
Parents need help!
What is also striking about these diseases is that up to 9 in 10 cases are thought to be preventable. Thus, concentrating on prevention rather than ‘cure’ makes most sense as the only economically feasible solution lies here. No single public health intervention is going to solve all the problems that the UK health system faces currently but one thing that has always stared me in the face was how clueless and/or irresponsible most parents are, regardless of which socio-economic stratum they belong to – writing this sentence as I read an article on a teenager who died from obesity after his mother continually brought takeaway to his hospital bed5. The consequence is children living through many traumatic experiences, picking up bad habits and developing health problems due to a combination of ignorance, lack of guidance and toxic environments.
A wise man was once asked: “How do we educate our children?” and he is said to have replied “Educate yourself as they will imitate you”. As a new father, I got to observe first-hand that my child is virtually learning everything in life from myself and my wife. Thinking back, my parents never smoked, did not allow any visitors to smoke in the house, and kept me away from friends who smoked. Their actions were the main factor for myself and my three siblings to never start smoking – although there was pressure from my school friends. Research suggests that this is true across the general population, that is, if parents do not smoke, their children are more likely to become adults who will not either6; if parents prepare healthy food, their children will do too; if parents do not drink or drink moderately, the children will do too; if parents are educated, their children will be too7; and the list goes on… As the only economically feasible hope seems to be prevention, there is no better place to start than educating parents.
Since starting as a researcher at my current institute, I have been to a dozen or so ‘induction courses’, taking lessons on a variety of subjects from ‘equality and diversity’ to ‘fire safety’ to ’unconscious biases’. Although most seemed a bit of a time waster at first, after enrolling to them, I soon accepted that these were important as I did not know how crucial they were in certain situations – situations that are more common than one would think. I would not have attended them if they were not mandatory.
However, arguably, none of these skills that I picked up in these induction courses are as important as being a good parent and helping my children achieve their potential physically, intellectually, psychologically, emotionally and socially. I think it is irresponsible that there exists no mandatory training before people become parents. We as parents are expected to be not just people who keep our children alive by providing for them, but we are also expected to be good dieticians, sleep coaches, pedagogues, psychiatrists, life coaches, friends… Unsurprisingly, many parents are failing horribly as we are not equipped with a solid foundation to guide them properly. The result is: one-third of the population is obese, one-fourth drink above advised thresholds, one-fourth of students report to have taken drugs, one-fifth smoke (noting that vaping is not included in this figure), one-fifth show symptoms of anxiety or depression and up to one-tenth may be game addicts.
To help parents in this long and extremely difficult journey of parenthood, I propose mandatory courses tailored for first-time parents – with exemptions & alternatives available. The specific syllabus and the length of the course should be shaped by pedagogy, public health, psychology, sociology, and epidemiology experts but also by the parents themselves.
In this course parents can:
Be persuaded about the importance of such a course – just as I learned that spending time learning about fire safety was not a bad idea
Be provided with links on where to easily find reliable information (e.g. NHS website)
Learn about the mental and physical health aspects of smoking, drinking alcohol, exercising, eating high sugar content food, pollution, watching TV, reading books, cooking healthy food, mould, asthma triggers, excessive use of social media etc.
Feedback any problems they have to a central panel and make suggestions as to how the course could be improved
Hear about local activities (e.g. ‘Stop smoking’ events, English courses, even events such as Yoga classes)
Receive information about who they can contact if they themselves have addiction problems (e.g. smoking, alcohol, drugs, gambling)
Learn about what to look out for in their children (e.g. any obvious signs of physical and mental diseases, bullying)
Be encouraged to support their children achieve their potential – no matter what background they come from
Be encouraged to offer help in local as well as national problems such as the organ donor shortage, climate change (recycling, carbon emissions), air pollution etc.
Be reminded of the responsibility to provide future generations a sustainable world
Be taught about the relevant laws (e.g. child seat, domestic abuse, cannot leave at home on their own).
I believe if the course is designed with the help of experts but also by parents, the course can be engaging and lead to more knowledgeable parents. This is turn will lead to positive changes in behaviour and a significant drop in the incidence of unhealthy diets/lifestyles, (at least heavy) smoking, substance use and binge drinking – major causes of the abovementioned common diseases. I think to ensure that parents engage and take part in the process, an exam should be administered where individuals who fail should re-take the exam. Parents who contribute to the process with feedback and suggestions can be rewarded with minor presents or a simple ‘thank you’ card from the government itself – a gesture that is bound to make parents feel part of a bigger process. Parents who are engaged in this process will also be encouraged to engage with their children’s education and help their teachers when they start going to school. Parental participation in turn, will positively affect academic achievement and the healthy development of children – a phenomenon shown by many studies8,9. Incentives such as additional child tax credit/benefit and/or paid parental leave for both parents should be considered to increase true participation rates.
These courses can then be accompanied by a number of optional courses where NGOs and volunteers from the local community can offer advice on matters such as ‘how to quit smoking?’, ‘how to find jobs?’, online parenting, English language courses (for non-speakers), and engaging children with local sports teams. I would certainly volunteer to give a session on the genetic causes of diabetes and obesity – and I know there are plenty of academics and professionals (e.g. experienced teachers, solicitors) out there whom would happily offer free advice to those who are interested. There are NGOs providing information on almost all diseases and health-related skills (e.g. CPR, first-aid) and this course would offer a more targeted and cost-efficient platform for them to disseminate their brochures and information on their upcoming events.
Many upper-middle to upper class parents regularly attend similar courses and events – and making this available to every parent would represent another way to close ‘the gap’10. Old problems persist but new ones are added on top such as online gaming, e-cigarettes, FOMO and betting addiction – and the courses can evolve with the times. A government which successfully implements such a course can leave a great legacy as social interventions have long lasting impact and even affect other countries.
One could argue that a course like this should be offered to every citizen at few key stages in their lives (e.g. first parenthood, before first child reaches puberty) – and that would be the ultimate aim. But as this option may initially be very costly and hard to organise and focusing on parents ensures that not only the parents are educated but consequently the children are too – making the process more cost efficient. The first courses could be trialled in certain regions of the country before going nation-wide.
We are all in the same boat – whether we realise or not
I would like to diverge a little to mention the potential sociological benefits of the proposed course: Tolstoy, in Anna Karenina wrote “Happy families are all alike; every unhappy family is unhappy in their own way” – also an increasingly used aphorism in public health circles. However, I observe and believe that many of us are unhappy due to similar reasons: we all want to be listened to, understood and feel like we are being cared about. I believe the proposed course accompanied with an honest feedback system would be a great start in getting the ‘neglected masses’ involved in national issues.
I would like to finish by returning to the little story at the start. I believe that many parents, especially those from poorer backgrounds, give up trying for their children early on as they do not think that they or their children can compete against other ‘well-off’ individuals and therefore see no future for themselves. Their children and grandchildren also end up in this vicious cycle. But if they get to see first-hand in the proposed course that we all – rich and poor – start from not too dissimilar levels as parents and have the same anxieties about our children can also motivate us all to push a little bit extra and hopefully close the massive gaps that exist between the different socio-economic strata in the UK11 – and ultimately decrease the prevalence of the diseases that are crippling the NHS.
Further reading
Shork, N. 2015. Personalized medicine: Time for one-person trials. Nature. 520(7549)
Bluett et al., 2015. Impact of inadequate adherence on response to subcutaneously administered anti-tumour necrosis factor drugs: results from the Biologics in Rheumatoid Arthritis Genetics and Genomics Study Syndicate cohort. Rheumatology. 54(3):494-9
Mike Vuolo and Jeremy Staff. 2013. Parent and Child Cigarette Use: A Longitudinal, Multigenerational Study. Pediatrics. 132(3): 568–577
Sutherland et al. 2008. Like Parent, Like Child. Child Food and Beverage Choices During Role Playing. Arch Pediatr Adolesc Med. 162(11): 1063–1069
Sevcan Hakyemez-Paul, Paivi Pihlaja & Heikki Silvennoinen. 2018. Parental involvement in Finnish day care – what do early childhood educators say? European Early Childhood Education Research Journal, 26:2, 258-273
Jennifer Christofferson & Bradford Strand. 2016. Mandatory Parent Education Programs Can Create Positive Youth Sport Experiences. A Journal for Physical and Sport Educators. 29:6, 8-12
We – as a group – carried out the largest genome-wide association study to identify genetic variants that are associated with decreased lung function and increased risk of chronic obstructive pulmonary disease. We hope that our findings will ultimately lead to the identification of effective drug targets for COPD. Image source: University of Leicester
I remember reading somewhere that ‘if you get asked the same question three times, then write a blog post about it’. That’s what I’ve been doing so far, and the purpose of this blog post is the same: to try and provide an answer to a commonly asked question. (Important note: my answers are in no way authoritative and only meant for interested non-scientists)
As a ‘Genetic Epidemiologist’, I constantly get asked what I do and what my (replace ‘my’ with ‘our’, as I do everything within a team) research can lead to. Please see my previous post ‘Searching for “Breathtaking” genes. Literally!‘ and My Research page for short answers to these questions. In tandem to these, I am constantly asked ‘why we can’t find a ‘cure’ for (noncommunicable) diseases that affect/will affect most of us such as obesity, diabetes, cancer, COPD – although there are many scientific advancements?’. I looked around for a straight forward example, but couldn’t find one (probably didn’t look hard enough!). So I decided to write my own.
I will first try and put the question into context: We do have ‘therapies’ and ‘preventive measures’ for most diseases and sometimes making that distinction from ‘a cure’ answers their question. For example, coronary heart disease (CHD) is a major cause of death both in the UK and worldwide (see NHS page for details) but we know how we can prevent many CHD cases (e.g. lowering cholesterol, stopping smoking, regular exercise) and treat CHD patients (e.g. statins, aspirin, ACE inhibitors). However, there are currently there are no ‘cures’ for CHD. So once a person is diagnosed with CHD, it is currently impossible to cure them from it, but doctors can offer quite a few options to make their life better.
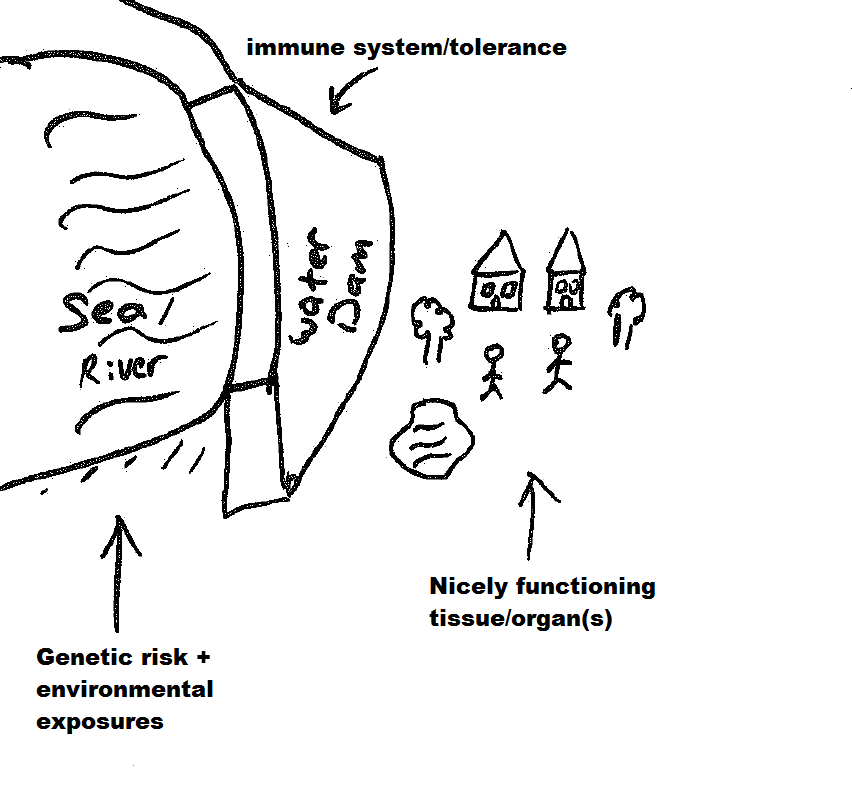
I then gave it some thought about why finding a ‘cure’ was so hard for most diseases, and came up with the below analogy of a river/sea, water dam, and a nicely functioning village/city (excuse my awful drawing!).
The first figure below sets the scene: there’s a water dam that’s keeping the river from flooding and damaging the nice village/city next to it. Now please read the caption of the below figure to make sense of how they’re related to a disease.
The river/sea is the combination of your genetic risk (e.g. you could have inherited genetic variants from your parents that increased your chances of type-2 diabetes) and environmental exposures (e.g. for type-2 diabetes, that would be being obese, eating high sugar content diet, smoking). The water dam is your immune system and/or mechanisms in your body which tame the sea of risk factors to ensure that everything in your body work fine (e.g. pancreatic islet cells have beta cells which produce insulin to lower your glucose levels back to normal levels – which would be damaging to the body’s organs if it stayed high).
So to ‘prevent’ a disease (well, flooding in this case), we could (i) make the water dam taller, (ii) make the dam stronger, and (iii) do regular checks to patch any damage done to the dam. To provide an example, for type-2 diabetes, point (i) could correspond to being ‘fit’ (or playing with your genes, which currently isn’t possible), point (ii) could correspond to staying ‘fit’, and point (iii) could correspond to having regular check-ups to see whether any preventive measures are necessary. Hope that made sense. If not, please stop reading immediately and look for other blog posts on the subject matter 🙂
Using the figure below, I wanted to then move to ‘therapy’. So as you can see, the river has flooded i.e. this individual has the disease (e.g. type-2 diabetes as above). The water dam is now not doing a good job of stopping the river and the city is in danger of being destroyed. But we have treatments: (i) The (badly drawn) water pumping trucks suck up excess water, and (ii) we have now built a second (smaller) dam to protect the houses and/or slow the flow of the water. Again, to provide an example using type-2 diabetes, water pumping trucks could be analogous to insulin or metformin injections, and the smaller dams could be changing current diet to a ‘low sugar’ version. This way we can alleviate the effects of the current and future ‘floods’.
Analogy for therapy/treatment – after being diagnosed with the disease
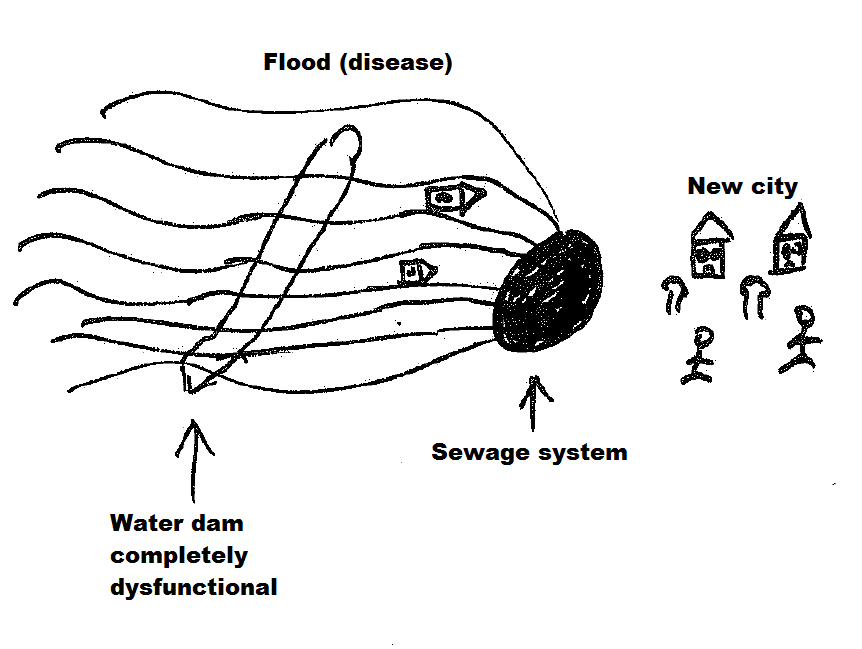
Finally, we move on to our main question: ‘the cure’. Using the same analogy as above, as the water dam is now dysfunctional, the only way to stop future ‘floods’ would be to design a sewage system that can mop up all water that could come towards the city. Of course the water dam and ‘old city’ was destroyed/damaged due to past floods, so we’d need to build a new functioning city to take over the job of the old one. A related real example (off the top of my head) could be to remove the damaged tissues and replace them with new ones. Genetic engineering (using CRISPR/Cas9) and/or stem cell techniques are likely to offer useful options in the future.
Analogy for cure – after being diagnosed with the disease
Hopefully it is now clear that the measures taken to prevent or treat the disease, cannot be used to cure the disease. E.g. you can build another dam in place of the old one, but the city is already destroyed so that’s not going to be of any use in curing the disease.
So to sum up, diseases like obesity, cancer, COPD are very complex diseases – in fact they’re called ‘complex diseases’ in the literature – and understanding their underlying biology is very hard (e.g. hundreds of genes and environmental exposures could combine to cause them). We’re currently identifying many causal variants but turning these findings into ‘cures’ is a challenge that we have not been able to crack yet. However, it is clear that the methods that we currently use to identify preventive measures and therapies cannot be used to identify cures.
I hope that was helpful. I’d be very happy to read your comments/suggestions and share credit with contributing scientists. Thanks for reading!
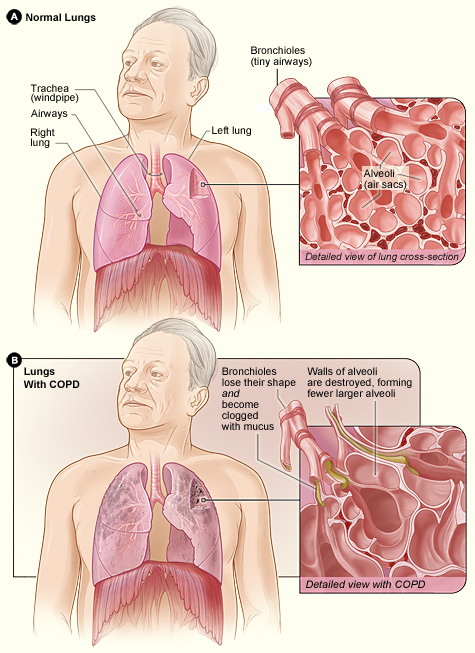
Difference between the lung of a COPD patient and an unaffected one. Image taken from the NHLBI website (one of the leading institutes in providing information on various diseases; click on image to access the source)
Many of us will either suffer or have a relative/friend who suffers from a disease called Chronic Obstructive Pulmonary Disease (COPD, click on link for details) which is a progressive respiratory disease characterised by decreasing lung function (struggling to inhale/exhale air, irreversible airflow obstruction), very likely accompanied by chronic infections. COPD has a prevalence of over 2% in the UK population (corresponding to approx. 1 million in the UK, probably a lower bound estimate due to many undiagnosed cases; this figure is approx. 16 million in the USA) and is currently the third biggest killer in the world (only behind cancers and heart-related diseases) – costing the lives of millions (in the USA alone, number of deaths attributed to COPD is over 100 thousand); and the health services, billions of pounds.
Contrary to the well-known genetic disorders such as Cystic Fibrosis and Huntington’s disease, which are diseases caused entirely by a person’s genetic makeup and caused by mutations in a single gene, COPD is a (very!) complex disease with many genes and environmental factors (e.g. smoking, pollutants) contributing to the development/progression of the disease. This complexity makes it much harder to dissect the causes and find potential (genetic) targets for cures or therapies. However, we do know that smoking is by far the biggest risk factor with up to 90% of those who go on to develop clinically significant COPD being smokers. But only a minority (<25%) of all smokers develop COPD, indicating the strong role genetics can play in the progression of this disorder. Also not all COPD patients are smokers (up to 25% in some populations), indicating that – at least in some patients – genetics can play a rather determining role. I must stress that all the statistics I provide here can vary considerably from population to population due to different lifestyles and genetic backgrounds.
I – together with a large group of collaborators – search for genetic predictors of lung function, which helps us to identify which individuals are more likely to develop the disease and potentially understand the underlying biology/pathology of respiratory diseases such as COPD and asthma, and related traits such as smoking behaviour. To do this, we carry out what is called a genome-wide association study (GWAS, click on link for details), where we obtain the genetic data (millions of data points) from tens of thousands of COPD (or asthma) patients and ‘controls’ (people with normal lung function). To ensure that our results are not biased by different ethnicities, life styles and related individuals, we collect all the relevant information about the participants and make sure that we control for them in the statistical models that we use. GWASs have been extremely successful in the identification of successful targets for other diseases and have led to the field of Genetic Epidemiology (GE, click on link for details) to come to the fore of population-based medicine. GE requires extensive understanding of Statistics (needed to make sense of the very large datasets), Bioinformatics (application of computer software to the management of large biological data), Programming (needed to change data formats, manage very large data), Genetics (needed for interpretation of results) and Epidemiology (branch of medicine which deals with how often diseases occur in different groups of people, and why); thus requires inter-disciplinary collaborations.
GWAS results are traditionally presented with a Manhattan plot (due to its resemblance of the city’s skyline) where the genetic variants corresponding to the dots above the top grey line (representing P-values less than 5e-8 i.e. 0.00000005) are usually followed up with additional studies to validate their plausibility. Image taken from Wikipedia (click on image to access source)
The inferences we make from these studies can shed light in to which genes and biological pathways play key roles in causing COPD. We then follow up these newly identified genes and pathways to analyse whether there are molecules which could be used to target these and be potential drugs for treating COPD patients. Our results can be of immense help to Pharmaceutical companies (and ultimately to patients), as many clinical trials initiated without genetic line of evidence have failed, costing the public and these companies billions of pounds.
As smoking is the biggest risk factor for respiratory diseases like COPD, I am – also with the contribution of many collaborators – in the process of analysing whether some people are more likely to start smoking, stop after starting, and smoke more than usual when they start smoking. The results can have huge implications as many people struggle to stop smoking, and when they do, research suggests that up to 90% (figure differs between populations) of them start to smoke again within the first year after quitting. Smoking is not only a huge contributor to the risk of developing COPD, but also to lung (biggest killer amongst all cancers), mouth, throat, kidney, liver, pancreas, stomach and colon cancer (not an exhaustive list). In the UK alone, these cancers cause the slow and painful death of tens of thousands, alongside a huge psychological and financial burden on the families and public resources.
The “lung” and the short of it (stealing a phrase thought up by my colleagues at the University of Leicester, click on link to see who they are) is that COPD is a disease that is going to affect many of us, and any useful finding which leads to cures and/or therapies could increase the life years of COPD patients and affect the lives of thousands of people directly, and millions indirectly (e.g. families of COPD sufferers, cost to the NHS). Finding targets to help people stop smoking can potentially have even bigger implications as many continue to smoke, despite huge efforts and funding allocated to smoking prevention and cessation.
A nice TED talk about the world of Data science and Genetic Epidemiology
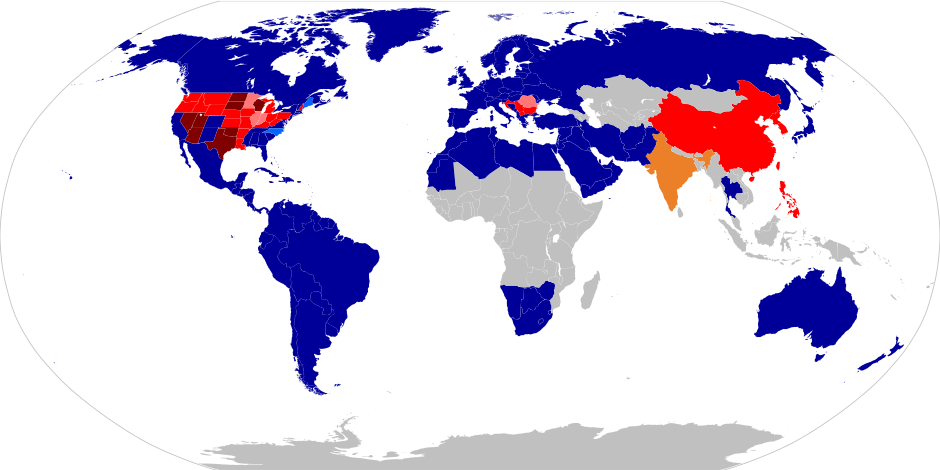
Laws regarding first-cousin marriage around the world. Navy blue: First-cousin marriage legal. Light Blue: Allowed with restrictions or exceptions. Yellow: Legality dependent on religion or culture. Red: Statute bans first-cousin marriage. Pink: Banned with exceptions. Dark Red: Criminal offense. Grey: No available data. The image has been released into the public domain by the author (URL: http://en.wikipedia.org/wiki/Cousin_marriage).
The answer is (studying) consanguinity (i.e. unions between relatives such as first-cousin marriages); and one cannot understand the complexity of the issue (and make ‘informed’ decisions) without reading the literature of these five apparently unconnected fields. It is fair to say that there is a degree of hostility towards consanguineous marriages in Western societies. However this perception is usually attained without in-depth knowledge on the genetic effects of consanguinity. In short, consanguinity per se (i.e. on its own) does not cause a disorder, but rather it increases the probability of an autosomal recessive disorder (which require two copies of the same) causal mutation to be in a homozygous state (i.e. possess two copies of the same mutation). When this happens both copies of the genes we inherited from our parents do not function properly.
Unions between individuals who are second-cousins or closer are considered ‘consanguineous’ in clinical genetics. Consanguineous families with diseases have been studied thoroughly by clinical geneticists for the last two-three decades – and this has allowed for identification of many disease causal genes. However, studying consanguineous populations as a whole rather than ‘cherry picking’ families with disease can offer much more for better understanding our genome and therefore finding new targets for preventive and curative medicine. Many genes in our genome still have unknown functions and we have merely scratched the surface in terms of their interactions. I hypothesise that assigning a function to the thousands of remaining genes will only be feasible if consanguineous populations are studied as a whole (i.e. also including families without disease to the studies) and I therefore carry out theoretical studies to estimate the sample size needed and how many genes will be completely ‘knocked-out’ if these studies were to be carried out. This approach proposes a ‘paradigm shift’ in clinical genetics.
Global prevalence of consanguineous unions. Consanguinity has deep roots in many cultures and it is impossible to interfere/intervene from the outside without first understanding why people engage in cousin marriages. Image source URL: http://www.consang.net/
Consanguineous unions occur very rarely in Western countries for a variety of sociological (e.g. cultural, negative media coverage) and statistical reasons (e.g. smaller families means fewer cousins at similar age), but the complete opposite is true in certain regions of the world where union of kin is seen as the default choice. Conservative estimates predict that approximately one-sixth of the world’s population (a figure of 1.1 billion is proposed by the Geneva International Consanguinity Workshop Report) live in highly consanguineous regions; and also another one-sixth falls into the ‘unknown’ category – reflecting the need for further research. Historically, consanguineous unions were also common amongst the elite in the UK (up to mid-19th century, including Charles Darwin), the Pharaohs and the Royal families of Europe (e.g. Habsburgs).
Views of main religions towards consanguineous marriages. NB: Where first-cousin marriages are allowed, lower levels of consanguinity are also allowed. Image Source: Copy-pasted from my own PhD thesis
The increase in the probability of a mutation being homozygous will depend on the level of relatedness between the parents. For example, approximately 6.25% of mutations are expected to be homozygous in the offspring of first cousins. This figure would be (near) 0% in the offspring of outbred individuals. Genetically, this is the main difference between union of kin and union of unrelated individuals. We all have many disease-causal mutations in our genomes (but in heterozygous state, i.e. one normal copy and one mutated copy) and different kinds of mutations are out there in all populations. However because these mutations will be very rare or are unique to you or your family, they do not get to meet their counterpart when you have offspring with an unrelated individual. Therefore the mutation’s homozygous effects are never observed. This is why rare autosomal recessive disorders are almost always seen in consanguineous offspring.
This difference in homozygosity levels is also one of the main reasons behind the necessity of studying consanguineous individuals and populations. These studies can turn unfortunate events (e.g. disorder in families) to a great use for medical sciences. Not only will identifying a disease-causal mutation help with diagnostics, they can enable scientists to understand what certain genes do and help us understand why the gene causes that disease. Rare instances can be highly informative about preventable outcomes relevant to the whole population. For example, had more notice been taken in the 1980s of the proof which familial hypercholesterolemia provided for the causal role of cholesterol in coronary heart disease (CHD), high cholesterol intake would have been better addressed for the nation a decade sooner. To provide numbers, CHD is still the UK’s biggest killer causing over 80 thousand deaths a year, thus paying more attention to information that was coming from studies of consanguineous unions could have saved thousands of lives just in this single case.
Given the advancements in genetic diagnostics (e.g. huge decreases in costs of DNA sequencing), screening for all known mutations will become feasible in the near future for everybody – and identifying disease-causal mutations will become even more useful for all of us. Our genomes are constantly being mutated and my approach will enable a much broader understanding of our genome by observing these mutations’ homozygous effects. Finally, rather than discourage (See link for an example) consanguineous marriages totally (not feasible in the foreseeable future due to many socio-economic and cultural reasons), for those willing to marry a cousin, screening for previously identified mutations will help these couples take more informed decisions.
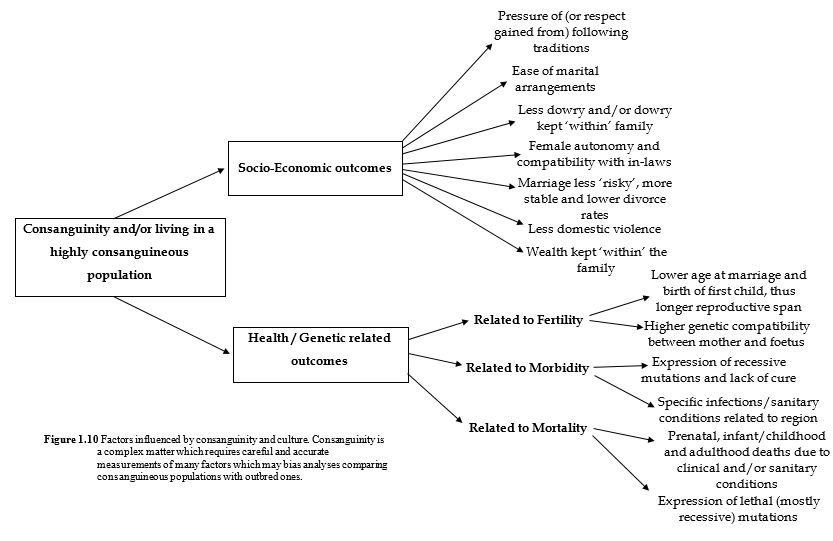
Factors influenced by consanguinity and culture. Image Source: Copy-pasted from my own PhD thesis (hence the Figure 1.10)
PS: Whilst the media is mostly responsible for portraying consanguinity the way they understand (and with more contrast added on of course), they could be forgiven as the genetic effects of consanguinity is not fully understood amongst geneticists either, especially in the field of complex trait genetics – thus the extra incentive for studying them.
Ben 12 yaşındayken (2000) ailecek İngiltere'ye taşındık ve ingilizcem neredeyse sıfırdı. Bunu duyan (Karen Holman adında) Sınıf Öğretmenim, kendimi evimde hissedeyim diye tüm arkadaşlarıma Türkçe cümleler dağıtmış. Sınıfa girer-girmez arkadaşlarımın hepsi bana "Hoşgeldin" dediler